

It’s 6 p.m. in Farin Shinge, Niger State. Inside a local medicine store, its lone fluorescent bulb defiantly flickers against the encroaching dusk. The vendor, Obi, squints at a faded thermometer, its mercury barely visible. A young woman, her infant whimpering with fever, sits on a rough wooden bench, eyes fixed on Obi with a silent plea for knowledge he barely possesses. His pharmacopoeia consists of basic antimalarials, a handful of pain relievers, and years of guesswork. Here, diagnosis is a gamble and treatment, a roll of fate.
A thousand kilometres south, in a well-lit, air-conditioned Lagos State University Teaching Hospital consultation room, a doctor engages an AI-powered system diagnosing breast cancer. The screen, glowing with precise probabilities, paints a future of predictive health, rapid intervention, and individualized treatment plans. Its algorithm, trained on global datasets, analyzes genomic markers, lab results, and patient symptoms.
This promise, however, clashes with Nigeria’s systemic healthcare reality. This dichotomy, replayed daily across Nigeria’s urban and forgotten rural communities, exposes the uncomfortable truth at the heart of this investigation. While discussions of technological advancements in healthcare are undeniably strong, the realities of remote communities starved of basic infrastructure and dealing with a gaping digital divide reveal a far more serious problem. This issue, far more than technological, is a national crisis that demands a deeper look.
An Ailing Nation
Decades of chronic underfunding, a devastating brain drain of medical professionals, and crumbling infrastructure deny millions of Nigerians basic healthcare access. For over 70% of Nigeria’s rural population, primary healthcare facilities are dilapidated shells devoid of essential drugs, functioning equipment, or even qualified staff, often lacking basic electricity or running water.


This void is made significantly worse by a doctor-patient ratio that hovers around 1:5,000 and can be higher in remote villages, leaving communities reliant on untrained medicine vendors and unlicensed healthcare providers. The tragic consequence is that Nigeria disproportionately bears the global burden of preventable diseases, suffering high infant and maternal mortality rates.
Amidst all these, proponents of AI argue for a future where AI-powered diagnostics enhance accuracy, telemedicine bridges geographical gaps, and predictive analytics strengthen public health responses. They insist AI could empower medical professionals, providing them with tools to make faster, more informed decisions, freeing them from clerical burdens, and extending their reach without replacing the human touch.
The Digital Void Where AI’s Promise Fades
This investigation, spanning rural communities like Farin Shinge and Kawo in Niger State, Sarsan in Kebbi State, and Ajiolo in Kogi State, reveals an often overlooked barrier standing between AI’s promise and its real-world impact in Nigeria: the digital divide.

“What is this AI you talk about to someone who can’t even charge their phone for two days?” asks Mallam Garba, a community leader in Kawo, Niger State. “We have no consistent electricity here. Our phones are for basic calls when there is network. The thing you talk of is a faraway dream for people like us.”
Mallam Garba’s frustration is commonplace and rational. Access to reliable electricity, a basic prerequisite for any digital technology, remains a distant reality for generations. According to the World Bank, over 80 million Nigerians lack access to the national grid, relying instead on expensive, noisy, and polluting generators or simply living in perpetual darkness. Without power, devices cannot be charged, internet modems cannot function, and AI systems, whether cloud-based or requiring local processing power, become useless. Even if a sophisticated AI diagnostic tool were somehow delivered to the primary health centre in Kawo, it would be an expensive dust collector.
Internet connectivity, while also improving nationally, remains painfully slow and too expensive in rural areas. “The 4G masts are in the towns, where the money is,” explains a health worker at Model Primary Health Care Centre Ajiolo in Kogi State who wishes to be anonymous. “Here in Ajiolo, we are lucky to get 2G, sometimes nothing at all. How do you run high-resolution image diagnostics or real-time video consultations with a doctor on that kind of bandwidth? Sending even a single photo on WhatsApp can sometimes take half an hour. For now, it is just impossible to deliver modern digital healthcare here.”
The cost of data and smart devices further worsens the problem. While urban dwellers might afford smartphones and data plans, the average daily income in many rural areas barely covers food, let alone the recurrent cost of digital amenities. This creates a two-tiered healthcare system before AI even enters the equation: one for the digitally connected, largely urban elite, who can benefit from AI’s advancements, and another for the majority, who are digitally disenfranchised and left behind in the dark.
Algorithmic Bias and Data Privacy Breaches
In addition to the infrastructure deficit, this investigation reveals a more significant, yet less visible threat: the ethical complexities of AI deployment in a diverse and rapidly developing nation like Nigeria. The promise of AI is often predicated on universal applicability, yet human diversity and local context are its missing links.
“When the data in the new environment does not match the patterns from the old environment, the model’s performance can degrade dramatically and unpredictably,” explains Engr. Busayo Adebiyi, a lecturer in the Computer Engineering Department of the Federal University Lokoja. “In other words, the data will be biased if it was trained on a particular context and applied to another.”


Engr. Adebiyi further explains that applying an AI model trained in one setting to another without careful adaptation can have negative implications because AI is a pattern-recognition system. “For instance, if symptom checkers or chatbots are not trained on local dialects, cultural nuances of symptom expression, or common local diseases like malaria, Lassa fever, or typhoid, unique to Nigerian epidemiology, they can provide misleading and potentially fatal advice. This is because AI models are not intelligent in the human sense.”
Then there is the issue of data privacy, one made more dangerous by low digital literacy and poor regulatory frameworks. As AI healthcare platforms gain traction, the question of user data security becomes paramount.
“When you upload your symptoms, your medical history, perhaps even images of your body, where does that data go? Who has access to it? And for how long will it be retained?” asks Barrister Odoma Uwodi, a rights advocate based in Lokoja. “Nigeria’s data protection laws are still nascent, and enforcement is often weak. Many of these platforms operate with privacy policies that are dense, opaque, and entirely incomprehensible to the average user, let alone an illiterate farmer in Kogi State who is simply trying to get help for his sick child.”
Nigeria’s 2023 Data Protection Act (NDPA) empowers the Data Protection Commission (NDPC) to ensure lawful and secure data processing, safeguarding citizen rights. However, practical implementation faces significant hurdles, particularly in the burgeoning health tech sector.
Health tech applications, for instance, commonly rely on broad consent for data aggregation and sharing, often involving commercial third parties. IT expert Eze Hanson considers such broad consent “necessary for product development.” Mr. Uwodi counters, questioning how “truly informed consent be obtained from those who don’t understand the technology or the implications of sharing their most sensitive health data? The concept of ‘tap to agree’ is meaningless when digital literacy is very low.”
Hope and Hesitation
In Sarsan, Kebbi State, the idea of AI assistance evokes mixed reactions, true to the complex relationship between desperation for care and deep-rooted skepticism. “If it means a doctor can see my child when there is no doctor at the primary health centre for weeks, then I will use it,” says Aisha, a mother of four. But her trust is conditional. “Who trains this clever machine? Does it know our sicknesses, our language? Or will it tell me I have a cough when my belly is swollen from dirty water?”
Aisha’s perspective accentuates the need for AI in healthcare to be culturally sensitive, linguistically appropriate, and locally relevant. Current models often fail to account for unique epidemiological patterns prevalent in Nigeria’s diverse regions or for the traditional health beliefs and practices that influence how people describe symptoms and seek care. Without data from and about these communities, AI risks becoming another tool of cultural imposition rather than empowerment.
“There’s no denying that most foundation models today are built in the West and have little to no local context, especially in healthcare. Beyond local context, geography also plays a huge part in medication outcomes, which is why two people may not have the same response or reaction to all medications,” says Adeola Ayoola, CEO/Co-Founder of Famasi Africa, a Nigerian health-tech startup that connects individuals and businesses to pharmacies.
Acknowledging AI’s evolving stage, Ayoola emphasizes a refined approach to ensure safe, reliable, and personalized healthcare. “I believe the first approach is to empower professionals,” she explains. In Nigeria, where “pharmacies are already responsible for 70% of healthcare visits in the communities,” Famasi Africa leverages AI to augment their efforts. This “human-in-the-loop effort helps ensure we safely deliver AI in healthcare.” Looking ahead, Ayoola foresees “more efficient on-device models that combine patient context with a privacy-first approach so we don’t sacrifice privacy while innovating.”


Addressing concerns about the practicality of integrating AI, Ayoola asserts, “It’s not impractical. As a team, we leverage AI in our daily activities, and we have learned that AI is useless without strong human capacity. Just like technology is an enabler of capabilities, AI helps to reduce redundant activities to focus on the more impactful ones.”
She provides an example from Famasi Africa’s work: “Pharmacies previously spent an average of three hours weekly to track their inventory and manually predict ordering patterns. With AI, this same pharmacist saves time and simply moves into decision-making based on the predictive and forecast results from our pharmacy software, Dispensary, which combines sales insight with seasonal awareness and geographical context to help pharmacies ensure they always have essential medications for their communities.”
Paths to Equitable AI?
The promise of artificial intelligence in revolutionizing Nigerian healthcare offers unprecedented opportunities for diagnostics, treatment, and public health management. Yet, the path to equitable and ethical deployment is far from being clear. This investigation reveals that the journey hinges on an infrastructure revolution.
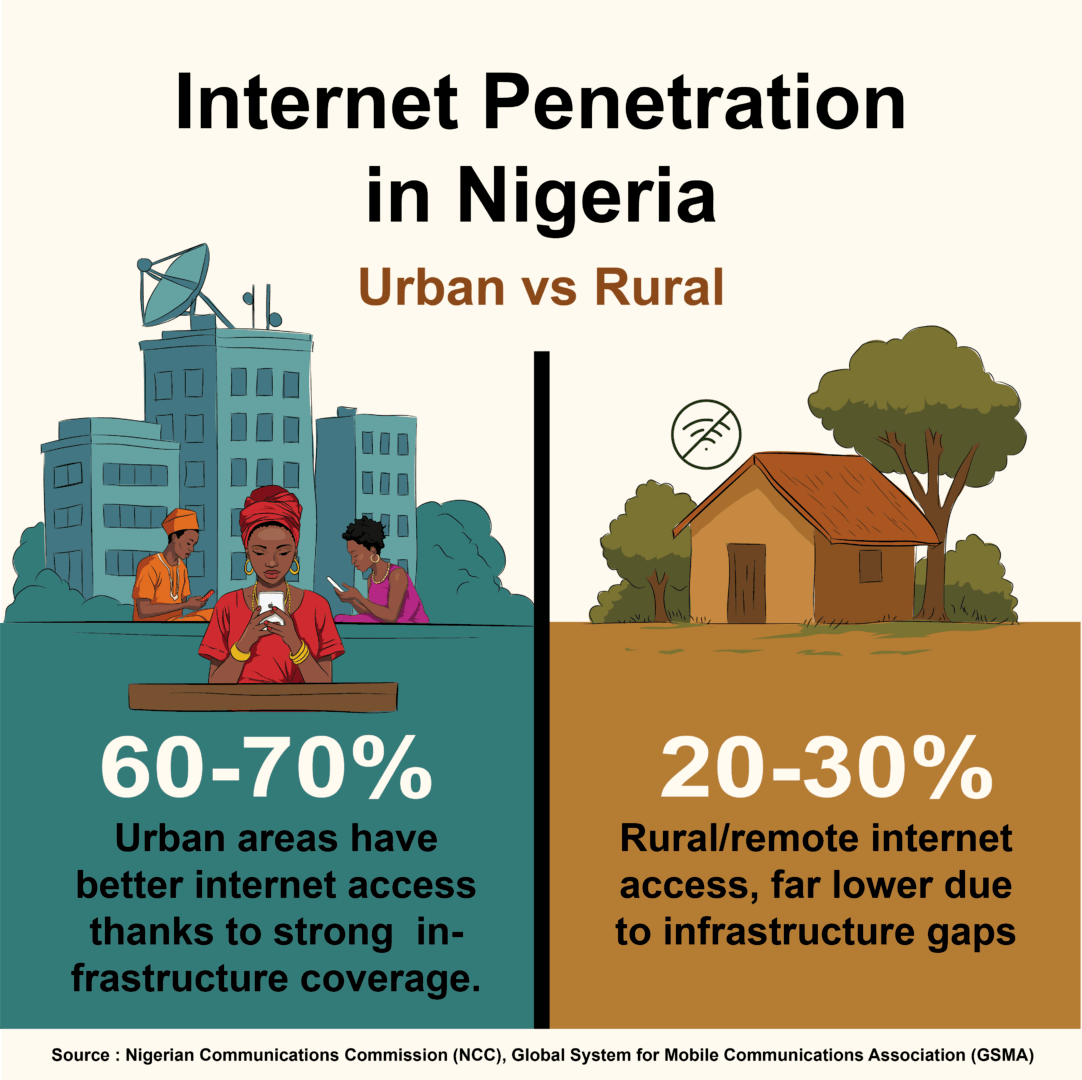
With only 45% of Nigerian households having access to reliable electricity and rural internet penetration being below 30%, stability for healthcare devices and the provision of affordable, high-bandwidth access are critically needed. “Without this foundational bedrock, even the most brilliant AI solutions remain theoretical, confined to urban centers and privileged institutions,” explains Hanson.
Nigeria urgently needs enforceable data protection laws specifically tailored to health data, accompanied by strong oversight mechanisms and clear penalties for breaches. Barrister Uwodi stresses that “Without clear ethical guidelines, transparent review processes, and simplified, locally translated consent mechanisms, public adoption of AI will be slow, perpetuating existing inequalities.”


To the very heart of the matter: AI solutions must involve the collection of extensive local, diverse Nigerian datasets with informed consent and anonymization, as well as intuitive interfaces accessible even to those with low digital literacy. Adekunle Omolabi, Program Officer at Youths in Justice Health and Sustainable Social Inclusion, argues, “It’s not enough to hand over a tablet; we must teach critical thinking about data privacy and AI’s limitations. This will empower communities to become active participants, not just passive recipients, ensuring solutions address local diseases rather than simply mirroring foreign models.”
AI for All Nigerians
AI holds transformative power, a tool capable of augmenting human intelligence and revolutionizing healthcare. The vision of a future where a smart algorithm empowers Obi in Farin Shinge or gives Mallam Garba’s Kawo community access to specialized medical advice is achievable. However, for it to be a force for good, it must be deployed with ethical foresight, foundational infrastructure, and a commitment to inclusivity.
“By investing in data infrastructure, developing strong governance frameworks, and building human capacity, Nigeria can unlock the transformative potential of AI to create a more equitable and accessible healthcare system for all its citizens,” Engr. Adebiyi succinctly concludes.
This report was produced with support from the Centre for Journalism Innovation and Development (CJID) and Luminate.